Study area
A cross-sectional study was conducted from June to August 2024 in primary schools in Thasala District, Nakhon Si Thammarat Province, covering an area of approximately 375.53 square kilometers. Thasala is a coastal district along the Gulf of Thailand and is divided into 10 sub-districts. The topography consists of both sandy and clay soils, with most of the population engaged in agriculture16. In this study, six sub-districts were selected: Taling Chan, Klai, Thai Buri, Thasala, Moklan, and Don Tako. The selected areas were based on similar geographical characteristics: Klai and Thasala are adjacent to the sea; Taling Chan and Thai Buri are on similar longitudes with Klai and Thasala, respectively, so they can be compared; and Moklan and Don Tako are non-landlocked. This selection allowed for geographical diversity while ensuring that some sub-districts shared similar characteristics, making the study comprehensive and spatially balanced as show in Fig. 1.

Sources: Esri, TomTom, Garmin, FAO, NOAA, USGS, OpenStreetMap contributors, and the GIS User Community. For more information about Esri software, please visit http://www.esri.com. All other layers were produced by the authors and are copyright-free.
The study area, which includes six sub-districts in Thasala District, Nakhon Si Thammarat Province: (1) Taling Chan, (2) Klai, (3) Thai Buri, (4) Thasala, (5) Moklan, and (6) Don Tako. Map was modified from Wikipedia Commons: https://en.wikipedia.org/wiki/Tha_Sala_district and ArcGIS software by Esri.
Sampling and sample size
A simple random sampling method from selected six sub-districts was used. Children, who had not received anthelminthics in the three months before attending the study, were included for screening of STHs infections. The sample size was calculated using the formula for estimating a finite population proportion17. Based on a prevalence rate (p) of 16%10, with a 95% confidence interval (z = 1.96) and a margin of error of 5% (d = 0.05), the estimated number of students aged 6–12 years was 10,71118. To allow for a drop-out rate of 25%, 254 individuals were required. However, a total of 319 participants had returned the assent and informed consent forms, so we included all individuals in the study.
Stool sample collection and STHs detection
A clean, labeled stool collection container with a scoop attached inside was distributed to all students who consented to participate a few days prior to specimen collection. On the day of container distribution, we provided verbal instructions using age-appropriate language and supplied documentation with clear illustrated protocol suitable for their age group. Students were instructed to take the containers home and collect stool samples according to the provided guidelines. They were directed to collect approximately 5–6 g of their morning stool specimen using the provided scoop and place it in the container, avoiding contamination with urine, water, or soil. To ensure proper handling, parents or guardians were informed about the study through written consent forms and were requested to assist their children with the collection process when necessary, following the enclosed instructions. The students then returned the samples to their schools, where our staff collected and transported them to the Medical Technology Laboratory at Walailak University for intestinal parasite detection.
We employed two highly accurate laboratory techniques to maximize the detection of parasites: FECT and APC. The FECT is highly sensitive, capable of detecting minimal quantities of parasites, particularly helminth eggs and larvae. The APC method cultivates parasites on agar plates to observe nematode growth, thereby enhancing the sensitivity for detecting S. stercoralis and/or hookworm infections. The preparation of stool samples and parasite detection protocols were conducted as previously described19,20.
Questionnaire survey
The questionnaire was administered by both the children and their parents, depending on the child’s ability to read and understand the questionnaire. For children who were unable to read, typically younger children in grades 1–3, a parent or guardian was instructed to complete the questionnaire on their behalf. This ensured that data collection remained accurate and comprehensive, regardless of the child’s ability to read. The questionnaire, adapted from previous research, was designed to evaluate various factors potentially associated with parasitic infections10. It included questions covering demographic information (gender and grade level), personal hygiene practices (handwashing, vegetable washing, and consumption of thoroughly cooked food), environmental behaviors (barefoot walking, toilet usage, and filtered water consumption), and risk behaviors (finger biting, interaction with pets, and nail trimming).
Statistical analysis of STHs infections and risk factors
Demographic data were presented using percentages and participant counts. The prevalence of STHs infections calculated by the number of infected children divided by a total of sample collection at time point multiply one hundred. The association between STHs infections and related factors was examined using Fisher’s Exact Test. Statistical test was considered significant at a p-value of less than 0.05. All analyses were performed using STATA package version 10.1 (StataCorp LLC, College Station, TX, USA).
Development of a predictive model to identify high-risk areas
Our study developed an innovative predictive model that integrates CNNs for land-use classification with ANNs that process PCA-refined data (Fig. 2). We employed CNNs for land-use classification using publicly available datasets from the USGS National Map Urban Area Imagery collection (21 classes, 100 images per class at 256 × 256 pixels)21. Model robustness was enhanced through image augmentation techniques including 90-degree rotations, averaging filters, noise introduction, and sharpening. We evaluated three CNN architectures22namely custom-designed CNN, ResNet50, and DenseNet121, using consistent hyperparameters and assessed their performance through accuracy, precision, recall, and F1-score metrics. The best-performing model was exported with optimized parameters to establish a foundation for the next step. Using a pre-validated classification model, we analyzed 30 satellite images from six schools (5 images per school) (Fig. 3), extracting unique architectural and locational parameters. This approach demonstrates how remote sensing and machine learning can enhance educational infrastructure analysis. All images were standardized to a resolution of 256 × 256 pixels to maintain uniformity in spatial resolution and facilitate comparative analyses across the dataset. To correlate satellite image parameters with STH prevalence, we integrated PCA with ANN. Our field survey-confirmed prevalence data and school parameters were combined and expanded using low variance noise. PCA reduced dimensionality (0.95 explained variance), with principal components feeding into an ANN for prevalence prediction. For area scanning, we established precise latitude-longitude boundaries with optimized step sizes to ensure comprehensive coverage. The well-trained CNN and ANN models worked collaboratively to classify regions, capturing both detailed features and broader patterns in satellite imagery. The resulting risk map was overlaid on original images, providing visual representation of spatial variations to support informed decision-making.
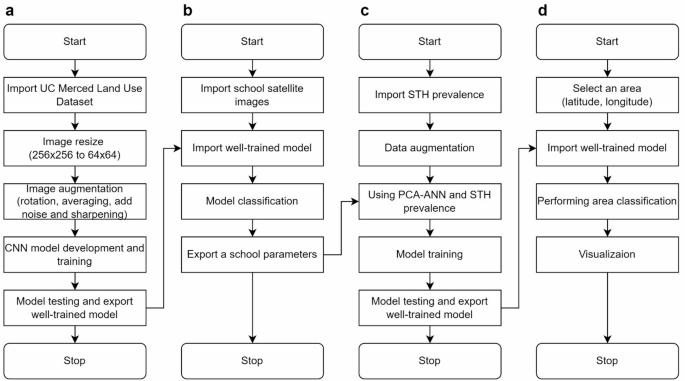
Four-stage satellite imagery analysis for STH transmission risk mapping. Our methodology includes: (a) CNN model development using UC Merced Land Use Dataset with image preprocessing; (b) Application of trained model to classify land-use patterns surrounding six schools in Thasala District; (c) Construction of a predictive model integrating parasitological diagnosis results with school environmental parameters; (d) Development of a geographic risk prediction system that generates spatial risk distribution visualizations based on coordinates.

Representative satellite imagery of six school campuses across different sub-districts in Thasala District used for predictive STH infection risk modeling: (a) Thai Buri, (b) Thasala, (c) Taling Chan, (d) Klai, (e) Moklan, and (f) Don Tako sub-districts. The satellite imagery was obtained and visualized using Folium version 0.19.5 (https://python-visualization.github.io/folium/) in the Python programming environment.
Ethics declarations
The study’s protocol was approved by the Ethics Committee in Human Research Walailak University (Approval No: WUEC-24-177-01). The study followed the Declaration of Helsinki. The study’s purpose and procedures were explained to the participants prior to enrolment. Written informed consent was obtained from all participants and the parent or the legal guardian of the child before the study onset. All study participants infected with STHs were treated with mebendazole or ivermectin.




