Trial design and setting
This intervention trial was registered on ClinicalTrials.gov on 21/11/2022 (Identifier number: NCT05623800).
The present study utilized a quasi-experimental design to evaluate the PREM-Kit. This study design was chosen due to geographical feasibility, where the intervention and control groups were drawn from two different campuses, with the intervention campus selected based on its proximity and accessibility to the researcher to facilitate regular monitoring, direct delivery of the educational sessions, and ensure fidelity of the intervention19,20. This trial was conducted in two campuses of a local public university, which are located 223 km apart. This intervention and data collection process lasted for 16 weeks, from 31st March 2023 until 31st August 2023.
Study population
The target population was late adolescents aged 18–19 years. The study participants were recruited from students taking the Health Science and Applied Science Diploma courses. They were chosen for the availability of the science module in the courses, wherein the HIV lecture was mandated in the curriculum (i.e. basic science and biology module) for standardization to minimize the selection bias between the intervention and control groups.
The inclusion criteria were students who attended the Health Science and Applied Science Diploma courses in 2023, late adolescents aged 18–19 years, and Malaysian citizens. Those excluded from the study were the students who refused to participate, those who were absent on the first session of the intervention, and those who did not understand the Malay language.
The present study applied a multistage sampling method to recruit the study participants. The first sampling stage was conducted to select campuses with science diploma courses. Two campuses were randomly selected from eight available campuses in the country through a simple random sampling technique. Both campuses were pre-assigned to study groups; the campus in the northern region of Peninsular Malaysia (Campus A) was selected as the control group, whereas the campus on the west coast of Peninsular Malaysia (Campus B) was selected as the intervention group. Next, the research team members conducted another simple random sampling to recruit the students in both groups. During the sampling of the students, the research team members were assisted by a field researcher in each campus to recruit the students using a students’ list performed by computer-generated software until the required sample size was achieved.
Sample size calculation
The sample size for this study was calculated by comparing two means using OpenEpi software21. The estimated difference in mean score between the intervention and control groups was selected based on a standard deviation from a previous local study with similar outcome measures22. Based on a power of 80% (β = 0.02), an alpha of 0.05, and a 20% attrition rate, the estimated difference in the mean knowledge score (0.4) yielded the largest sample size, which was 92 participants per group. Hence, the final calculated sample size in this study was 184 participants.
Intervention trial
This study provided an HIV education intervention delivered by the principal researcher using the newly developed PREM-Kit. The participants in the control group did not receive any active intervention except for their routine curriculum-mandated basic science and biology module encompassing subjects such as histology, biology, and infectious diseases. On the other hand, the participants in the intervention group were provided with the PREM-Kit intervention in addition to the curriculum-mandated basic science and biology module.
The PREM-Kit intervention was conducted in two lecture-based sessions using PREM-Kit’s flip chart (in a Microsoft PowerPoint slide) and PREM-Kit’s videos demonstration for six weeks. The first session delivered Module 1 (during the first visit) in Week 0, followed by the second session, which delivered Module 2 and Module 3 in Week 6 (Fig. 1). Each session was also accompanied by question-and-answer activities as open quizzes with prizes to stimulate participants’ engagement. Both sessions took approximately 30 to 60 min (30 min for each module).
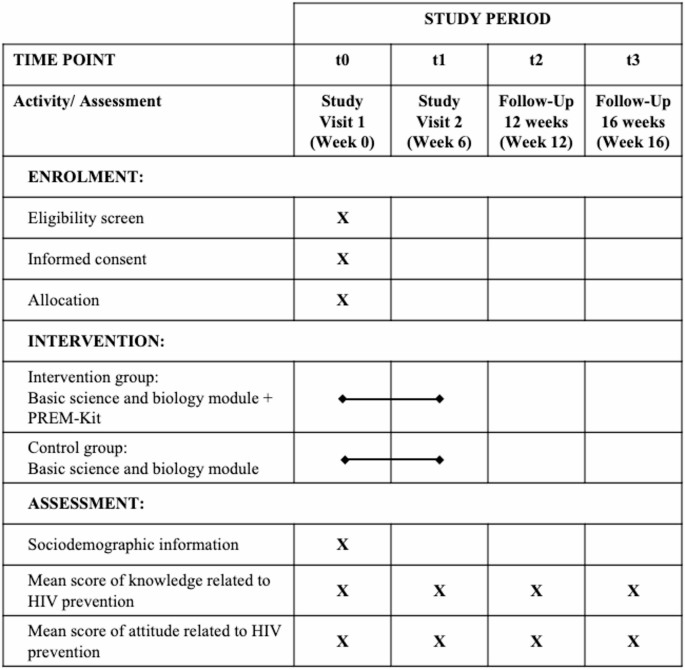
Schedule of enrolment, interventions, and assessments based on Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT 2023) Checklist.
Participants’ enrolment and assessment
The field researcher at each campus screened students who attended the selected campuses for inclusion and exclusion criteria. Eligible students were invited to participate in the study for a duration of 16 weeks, comprising both intervention and data collection. There were four time points of activities and assessments on knowledge and attitudes related to HIV prevention (Fig. 1).
At baseline (t0), we collected data on participants’ knowledge and attitudes related to HIV prevention and sociodemographic information. The first intervention session follows this assessment. Consequently, the second intervention session was carried out in Week 6. Upon completing this session, the participants were provided with a similar questionnaire to respond to the immediate post-intervention assessment (t1), followed by the 12-week post-intervention assessment (t2) and the 16-week post-intervention assessment (t3).
Measures
Sociodemographic characteristics
This study examined six independent variables, which were: (i) age of the study participant, (ii) sex of study participants, (iii) ethnicity of study participants, (iv) current place of living, (v) types of secondary school, and (vi) history of receiving HIV/sex education during secondary school.
Outcomes
The outcomes of the present study were measured in terms of knowledge and attitudes scores related to HIV prevention using a validated Malay version of a self-administered questionnaire of knowledge, attitudes, and practices (KAP) related to HIV prevention23. This instrument was pretested among Malaysian adolescents and had acceptable validity and reliability (Cronbach’s alpha coefficient = 0.61–0.73). The knowledge score is determined by calculating a mean score of knowledge at baseline, immediately post-intervention, 12 weeks post-intervention, and 16 weeks post-intervention. It consisted of 15 items with a “yes”, “no”, or “I do not know” response. The possible range of the knowledge score is 0 to 15, where a higher score indicates a higher level of knowledge. The attitude score is obtained by calculating the mean attitude score at baseline, immediately post-intervention, 12 weeks post-intervention, and 16 weeks post-intervention. It comprised eight items, each with a 5-point Likert scale (strongly agree, agree, undecided, disagree, and strongly disagree) for a response. The attitude score can range from 8 to 40, with a higher score signifying a more positive attitude towards HIV prevention. Data on practices related to HIV prevention was also collected. However, it was not presented in this paper.
Statistical analysis
To evaluate the intervention’s effectiveness, an intention-to-treat analysis approach was used to retain the participants in this study. Data were analyzed using the IBM SPSS Statistics for Mac, version 2624. All missing values were examined, and it was found that the final dataset (n = 187) contained missing values (knowledge and attitudes scores at t1-t3) ranging from 7.0% to 15.0%. Subsequently, we applied multiple imputation method to replace all the missing values because of (i) longitudinal data, (ii) the presence of more than 5% missing values, and (iii) Little’s MCAR test violated the assumption of missing completely at random (p-value = 0.027)25,26.
A baseline group comparison was performed by examining the sociodemographic characteristics of participants. Continuous data were presented using the mean (standard deviation). Besides, frequency (percentage) was used to describe the categorical data. An independent t-test was used to compare the distribution of continuous data to demonstrate the participants’ comparability between the intervention and control group. In contrast, the distribution of categorical data between groups was conducted using the chi-square test for homogeneity. As for variables with violated assumptions for the chi-square test for homogeneity, the continuity correction test was used. The level of significance for the statistical test was set at 0.05.
Repeated measure analysis of variance (RMANOVA) was applied to examine the changes of knowledge and attitude scores within a group, between groups and between groups over time, i.e., at Week 0 (baseline), at Week 6 (immediately post-intervention), at Week 12 (12-week post-intervention), and Week 16 (16-week post-intervention). Repeated measure analysis of covariance (RMANCOVA) was applied with baseline knowledge and attitude scores as the covariates. Mean (standard deviation) scores for each group, mean differences, F-statistics, degrees of freedom, p-values, 95% confidence intervals (CI), and partial eta-squared values were reported. The level of significance was set at 0.05. We included RMANOVA results in the Supplementary Table S1 and S2.




