From January 2012 to January 2023, we reviewed the data of all patients who underwent Masquelet technique treatment. Adult patients with FRI in the shoulder girdle (e.g., clavicle, humerus, and scapula) were included in this study. Inclusion criteria: patients diagnosed with FRI in the shoulder girdle; patients treated with Masquelet technique; age ≥ 18 years; ≥24-month follow-up. Other exclusions were applied for: palliative/amputation interventions, incomplete records, and comorbid malignancy. The diagnosis of fracture-related infection (FRI) was confirmed through a multidisciplinary evaluation meeting ≥ 1 of the following criteria1,2; (i) pathognomonic signs (e.g., fistula, sinus tract, wound dehiscence, intraoperative purulence), (ii) definitive microbiological evidence from ≥ 2 concordant deep-tissue cultures, or (iii) histopathological confirmation of microorganisms or infection-associated tissue changes. Demographic and clinical parameters were systematically documented. The institutional review board approved this retrospective study, and the investigation was conducted in accordance with ethical principles of research, the informed consent was waived as this is an observational cohort study.
We identified 62 patients (39 male and 23 female) with a mean age of 45.52 ± 14.01 years. Among which, scapular FRIs were excluded due to insufficient cases in our cohort (n = 0), finally included 8 patients of clavicle and 54 patients of humerus. Table I presents the basic data of these cases. Nine patients with shoulder girdle FRI were excluded from the study due to predefined criteria: three were under 18 years of age, one presented with Cierny-Mader (C-M) Host Type C infections (contraindicated for surgical intervention), three lacked the minimum required 24-month follow-up period, and two exhibited concurrent nerve injuries that could confound functional evaluations. Comprehensive preoperative data were systematically gathered, encompassing medical histories of prior trauma and surgeries, laboratory diagnostic results, imaging studies [e.g. radiography, magnetic resonance imaging (MRI), computed tomography (CT), and radionuclide bone scans], and physical examination records. The extent of debridement and selection of fixation strategies were guided by preoperative imaging assessments and intraoperative findings.
Surgical techniques
A standard staged Masquelet technique was performed11,12,13. During stage one, radical debridement was performed, with all septic, devitalized tissue and implants completely removed (Fig. 1). The debridement was performed using a high-speed saline-cooled burr to remove necrotic bone, and granulation tissue was debrided using a rongeur. The membrane was curetted from the bone bed, ensuring margins of healthy, bleeding tissue, including at least 5 mm of normal bone (both cortical and cancellous) and 2 mm of normal soft tissue, which align with established protocols for debridement of orthopaedic infection4,12. In patients with unstable fractures or defects, internal plate fixation was performed after radical debridement (Figs. 1, 2 and 3). Subsequently, the residual void was filled with an antibiotic-impregnated PMMA spacer (500 mg gentamicin per 40 g of PMMA powder, mixed with 4 g of vancomycin powder)12. Notably, the antibiotic cement completely coated the implant, if present. All patients were treated empirically with broad-spectrum systemic antibiotics when cultures were sent, and the regimen was adjusted to the responsible pathogen once the culture results were obtained. Postoperative intravenous antibiotics were administered for two weeks, followed by oral antibiotics for another four weeks5,18. Partial weight-bearing exercises were encouraged during this period.

Intraoperative view from a 24-year-old male with FRI in clavicle, treated with Masquelet Technique. (a)Multiple sinus tract in the wound in midshaft clavicle. (b) Plate fixation after radical debridement. (c) The antibiotic-coated cement spacer filled the bone defect and coated the plate. (d) Complete infection control and soft-tissue healing before bone graft in the second stage. (e) The cement was removed and protecting induced membrane in second stage, (f) then the defect was restabilized and with bone graft.
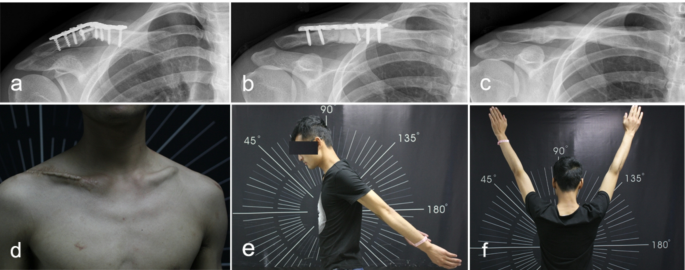
Imaging and functional results of a 24-year-old male with FRI in clavicle, treated with Masquelet Technique. (a)X-ray of a patient with FRI in midshaft clavicle. (b) Post-debridement X-ray with an antibiotic cement spacer and a plate for internal fixation. (c) X-ray of bone healing state 2 years after second stage bone grafting. (d) Functional result at the two-year follow-up showing good infection control and wound healing, (e) full stretch and full elevation of shoulder joint (f).
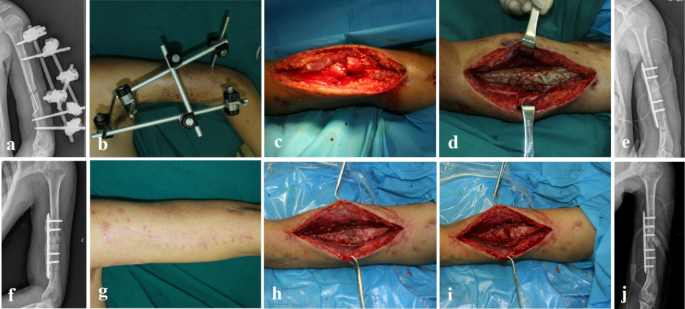
Staged surgical treatment of a 35-year-old male with FRI in humerus by Masquelet Technique. (a) Preoperative X-ray showing nonunion of midshaft humerus and an external fixture treatment. (b) Intraoperative view showing a wound exudation and an external fixator. (c–e) Remove external fixator, radical debridement, an cement spacer filled the bone defect and internal fixation with a plate. (f–g) Imaging and soft-tissue evaluation before bone graft in the second stage. (h–i) redebridement, replacing implant and bone grafting in second stage surgery.
During stage two (at least six weeks after debridement), the host’s condition was reassessed, including infection control and soft tissue healing. If there were no clinical signs of infection, normalization of the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), and adequate soft tissue healing, bone grafting was initiated. Deep tissues around the defect were sent for pathological analysis and bacterial culture to confirm infection eradication. If any persistent infection was found (e.g., the number of central granulocytes per high-power field exceeded 5)19revision surgery was performed. The cement was removed, and the unstable fracture or defect was restabilized. Bone grafting was based on the patients’ requirements, age, and the characteristics of the bone defect. According to standard technique8,9,10,11autografts were prioritized for bone defects due to osteogenic superiority. And no more than a third of the allograft is added to ensure bone healing in cases lack of adequate autograft. Cancellous bone was cut into 0.3 × 0.3 × 0.3 cm pieces and used to fill the defect adequately. Finally, the induced membrane pocket was sutured, and the wound was closed.
Follow-up and data collection
To evaluate the outcomes and functional results, treated patients had regular outpatient visits at 2, 6, 9, 12, 18, and 24 months after grafting. X-ray images were routinely taken to assess fracture healing. The primary outcomes were fracture healing and infection eradication. Bone union10,11,12 was defined as continuous callus bridging all three cortices on radiographic imaging. Recurrence of infection was defined as a relapse at the same site from which the infection had previously been eradicated, following the cessation of therapy and a period of infection eradication, in accordance with established diagnostic criteria for FRI1,2,18. A patient who had eradicated infection for 2 years post-treatment was classified as having achieved an “infection free”. Clinical assessment was performed by two independent, experienced trauma surgeons.
In addition, DASH score was used to quantify functional outcomes. Patient follow-up was conducted by full-time clinical research specialists, and complications were also recorded. The collected data included patient epidemiological characteristics and treatment-related parameters. The epidemiological characteristics of patients included age, sex, etiology, infection site, history of metalwork usage, presence of sinuses or open wounds, and comorbidities. Treatment-related parameters were derived from hospital medical records and included the preoperative C-M classification, surgical strategy, microbial characteristics, antibiotic administration, fixation methods, bone grafting, and the incidence of intraoperative complications.
Statistical analysis
Data were analyzed using the SPSS 22.0 statistical software package (SPSS Inc, Chicago, IL, USA). Continuous variables were expressed as the mean ± standard deviation (SD) and compared using an independent t-test or paired t-test. Categorical variables were described using frequencies and percentages, and were analyzed using the chi-square test or Fisher’s exact test, as appropriate. A p-value of less than 0.05 in a two-sided test was considered statistically significant.




